
Neurodivergence & Co-occurring Health Conditions
Co-occurring Conditions, Misdiagnosis & Barriers to Healthcare: The Reality for Neurodivergent Individuals
Those within the neurodivergent community have identified numerous health and mental health conditions that commonly co-occur with neurodivergence. Research is beginning to verify that these clusters exist, however there is still much to learn about the reason behind these links. Unfortunately, this emerging knowledge has not yet been integrated into common practice, resulting in further delay in identification of additional diagnosis and higher chances of misdiagnosis.
Physical differences or symptoms that are more common among neurodivergent people include:
- Fine & Gross Motor Difficulties
- Clumsiness/Poor coordination
- Musculoskeletal pain/Muscle weakness
- Generalised joint hypermobility
- Chronic pain
- Migraines/Frequent headaches
- Fatigue
- Sleep problems
- Fainting/Vertigo/Dizziness
- Heart palpitations/Racing heart
- Wheezing/Shortness of breath
- Constipation/Diarrhea/Stomach cramps
- Urinary incontinence/Urgency
- Abnormal temperature regulation
- Hives/Itchy skin
- Fragile/Stretchy skin
- Poor wound healing/Bruise easily
- Intense period cramps
- Pain during or after sexual intercourse
- Chronic pelvic pain
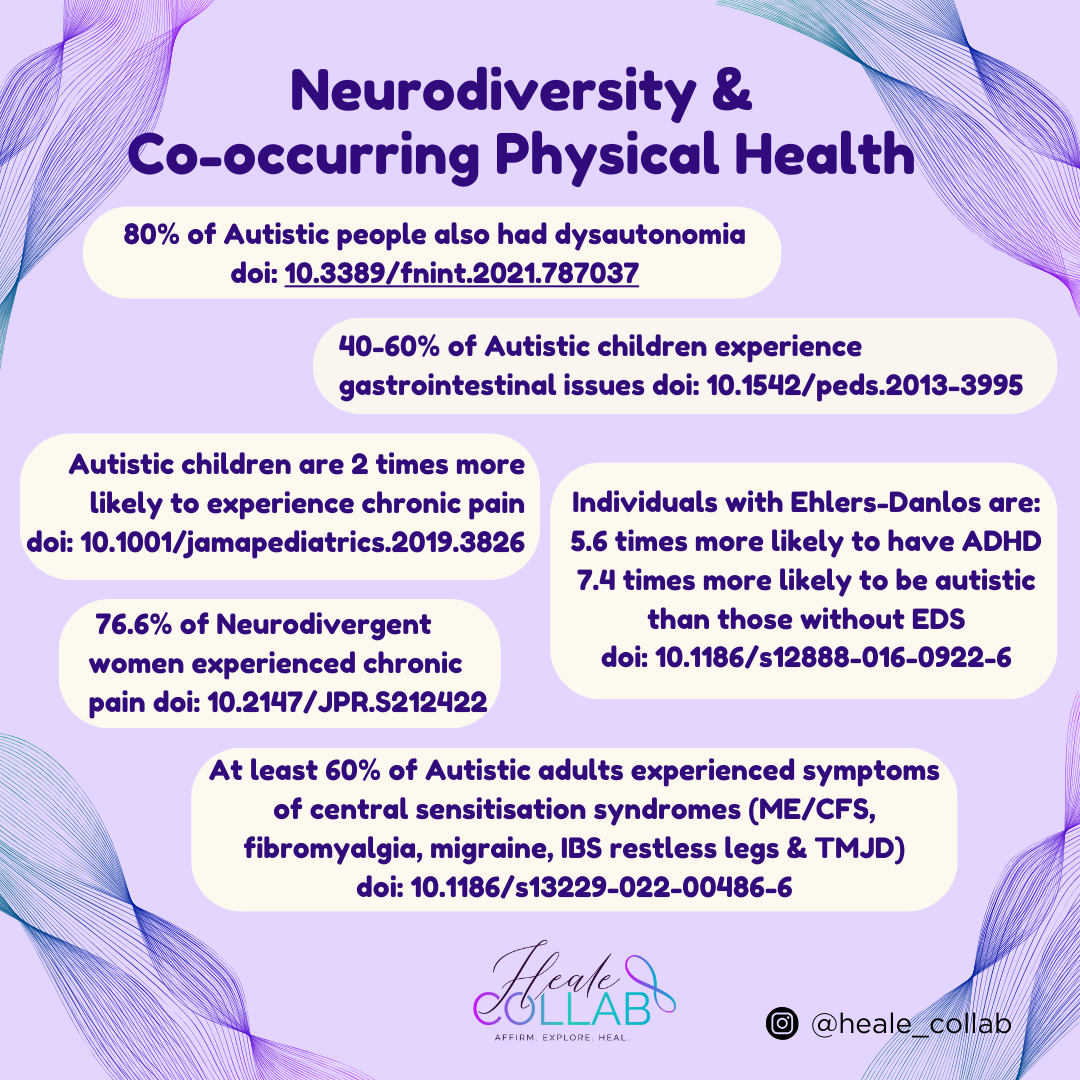
These symptoms can often be attributed to a range of conditions including Dysautonomia, Endometriosis, Mast Cell Activation Disorder, Fibromyalgia, and Connective Tissue disorders such as the Ehlers-Danlos Syndromes (EDS). Recent studies have shown that there are emerging links between Hypermobility, Neurodivergence, Dysautonomia, Fibromyalgia and Pain. Participants with a diagnosis of Autism, ADHD or tic disorder (Tourette syndrome) demonstrated elevated levels of hypermobility along with significantly more symptoms of pain and dysautonomia.[1] These studies also encouraged proactive screening of patients with fibromyalgia and hypermobility for neurodivergent traits and vice versa to facilitate diagnosis and management.[2]
There are also mental health conditions, neurodevelopmental disorders, and learning differences that are commonly identified as co-occurring among neurodivergent people including:
- Eating disorders (including ARFID & Binge Eating Disorder)
- Post-Traumatic Stress Disorder (PTSD)
- Substance Abuse
- Personality disorders
- Obsessive Compulsive Disorder (OCD)
- Premenstrual Dysphoric Disorder (PMDD)
- Anxiety
- Depression
- Rejection Sensitive Dysphoria (RSD)
- Sensory Processing Disorder (SPD)
- Auditory Processing Disorder (APD)
- Speech or Language disorders
- Learning disorders (including Dyslexia, Dysgraphiaand Dyscalculia)
- Twice exceptional (exceptional ability alongside disability)
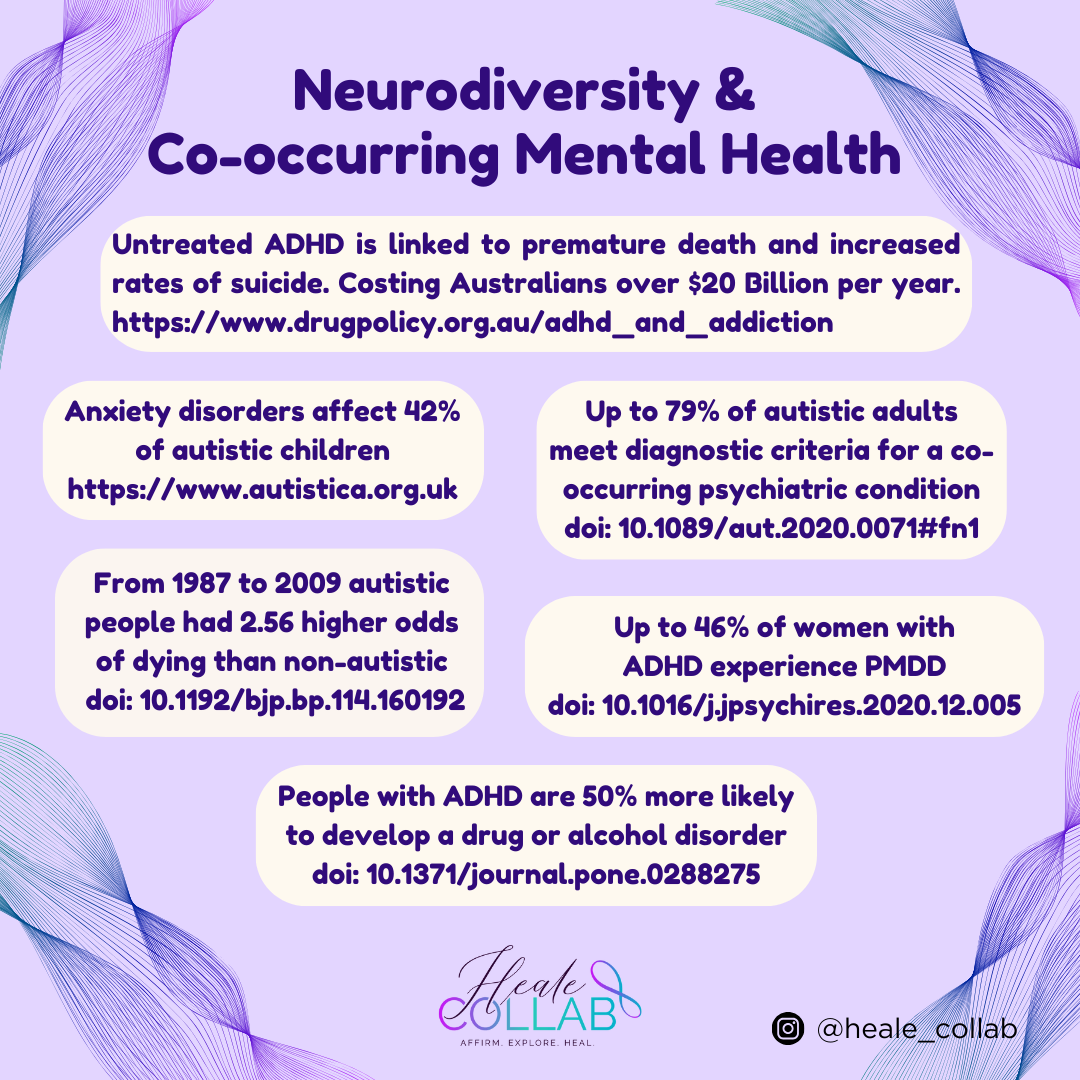
As with physical symptoms and conditions, many neurodivergent people will experience a variety of differences that can be attributed to combinations of the conditions listed above. Neurodivergent individuals commonly experience co-occurring Anxiety, Depression[3] and eating disorders.[4] A high prevalence of ADHD, Autism, Anorexia Nervosa, Addiction, Obsessive Compulsive Disorder, and anxiety disorder has been found in patients with EDS.[5] Adults with ADHD have been found to have higher rates of Mood Disorders, Anxiety Disorders, Substance Use Disorders (SUD) and Obesity than the general population.[6]
Recent studies suggest that Autistic & ADHD individuals have an increased risk of co-occurring SUD. While substance abuse may improve management of their symptoms in the short term, it has been found to generally worsen difficulties with daily functioning over time.[7] Evidence also suggests that there is an increased prevalence of ADHD in those presenting with SUD, and ADHD has a negative influence on the course of substance use disorders. There is currently a mistaken belief by some that the use of stimulant medication to treat ADHD may cause or increase the risk of later developing substance use disorders. This belief may result in people with ADHD not accessing or not being offered the most effective medication for ADHD, despite research having found stimulant treatment in people with ADHD can result in positive outcomes for those with co-occurring substance use disorders.[8] Greater interaction between addiction specialists and ADHD-specialists is urgently needed to ensure those with ADHD receive access to the most appropriate treatment.
Women and people assigned female at birth with ADHD or Autism are disproportionately affected by PMDD.[9] Women affected by EDS often present with significant gynaecological symptoms that are disabling, such as heavy menstrual bleeding, severe menstrual cramps, and painful intercourse.[10] Studies have also shown that women diagnosed with endometriosis are more likely to have ADHD, Depression, Anxiety, and chronic pain conditions like Fibromyalgia.[11] In Australia it currently takes on average 6 and a half years for those living with endometriosis to be diagnosed.[12] This is similar for many of the physical health conditions that co-occur with neurodivergence with it often taking a prolonged time for those with symptoms to receive an accurate diagnosis.
It has also been noted that neurodivergent individuals may be at increased risk of developing PTSD. Difficulties with emotional regulation can lead to heightened emotional responses, such as intense fear, anxiety, or anger. Due to sensory sensitivities, an event that is not upsetting to a neurotypical person may be completely overwhelming to an autistic person. Communication difficulties mean that verbal reporting and processing of the event may not be possible, which can lead to inadequate treatment and support.[13] The high co-occurrence of PTSD can result in a missed diagnosis, where PTSD is accurately diagnosed and then used to explain any Autistic traits, leaving Autism undiagnosed. When Autism is missed, the trauma treatment fails to be adapted with a neurodivergent approach, and the treatment will be negatively impacted.[14]
Dr. Neff from Neurodivergent Insights has written a whole series regarding misdiagnosis across neurodivergence and mental health conditions. This is in part due to many of the conditions sharing genetic, temperamental, and trait overlap as well as sharing psycho-social risks, such as victimization, substance abuse, disordered eating, mood disorders, PTSD, self-harm, and more. Even experienced clinicians who know these conditions well can find it difficult to differentiate at times. An example of this is how ADHD and Autism predispose people to personality disorders, including borderline personality disorder. In turn, borderline personality disorder can be a misdiagnosis for Autism or ADHD but most likely specifically in Autistic-ADHDers.[15]
Autistic Burnout is a relatively new concept that historically has most likely been misdiagnosed as Depression. Autistic adults describe their experience of Autistic Burnout as a long-lasting pervasive state of exhaustion, loss of function, and reduced tolerance to stimulus that arises from chronic life stress, a mismatch between expectations and abilities, and not having adequate supports. It substantially impacts on people’s lives, often resulting in loss of vocation, health, quality of life, and, at times, leading to suicidal behaviour. This is different from depression, as anhedonia and sleep problems are less prevalent in Burnout. Also lived experience reports that the experience of autistic burnout is different from an episode of depression, but that autistic burnout can contribute to subsequent onset or relapse of depression.[16]
There is a substantial amount of emerging evidence that demonstrate how interwoven neurodiversity, mental health, hormones, and physical health are. It is less clear what may be correlation versus causation and what the underlying explanation for these clusters of conditions is. A recent study[17] found that neurodivergent children are more likely to have hypermobility, pain related conditions, gastrointestinal concerns, continence issues and extreme tiredness. It also showed that these physical health problems often do not receive appropriate diagnosis or support due to clinicians not knowing about the increased co-occurrence, or assuming that the complaint is due to existing diagnoses.
Many neurodivergent adults speak about experiencing ongoing issues with their physical health that take many years to be correctly diagnosed (if at all). Autistic individuals have reported having their concerns dismissed by health professionals, or their health needs or disability being misunderstood.[18] Differences in interoception, as well as emotional and behavioural displays such as masking also contribute to misdiagnosis or no diagnosis. The impact of incorrect diagnosis can lead to further trauma due to being dismissed and then living without appropriate treatment.[19] The intersectionality of disability, mental health issues, gender or sexual diversity, cultural diversity, drug and alcohol use, and poverty can also impact healthcare accessibility.[20]
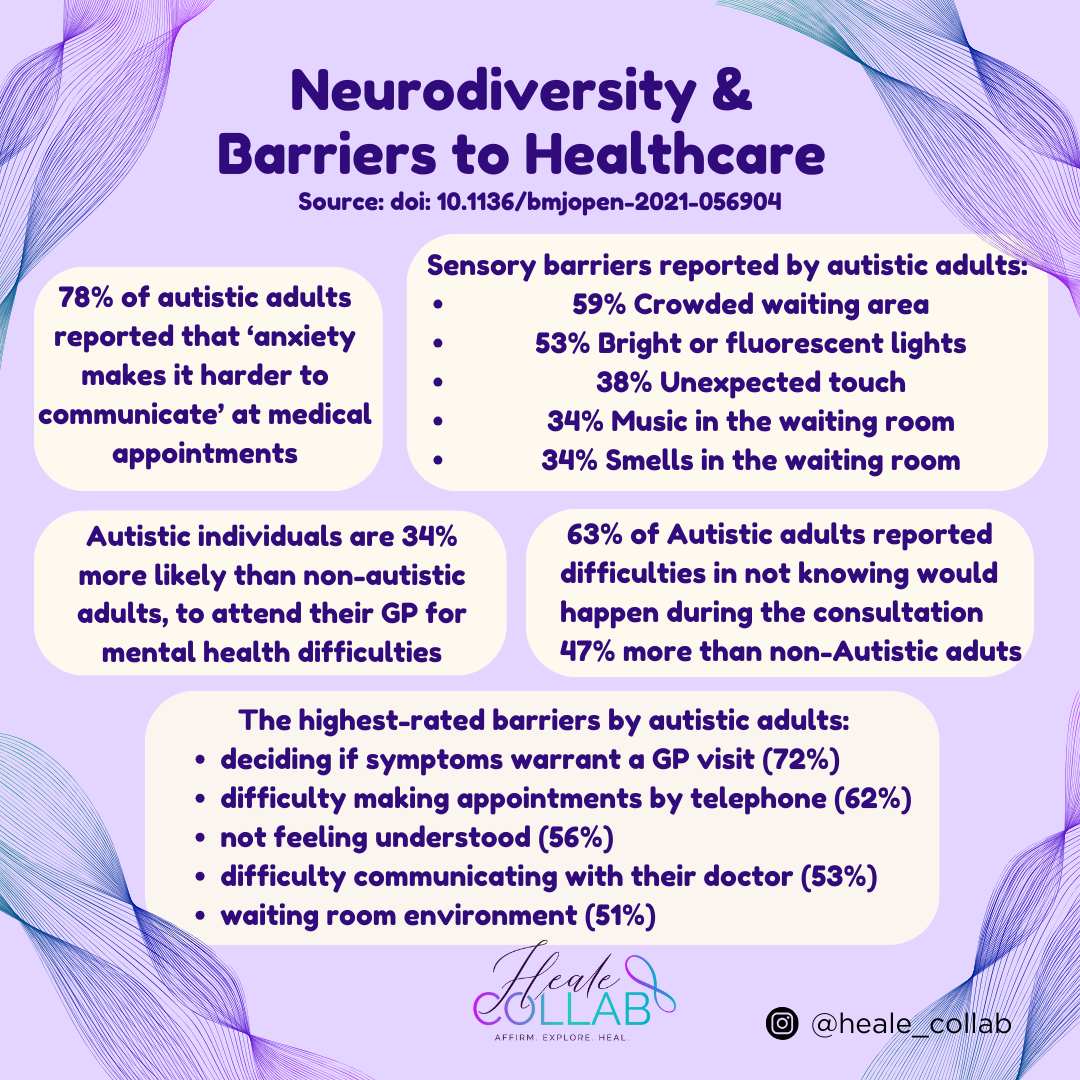
Barriers faced by autistic people engaging with healthcare include difficulties deciding when to seek care, reluctance to bother their GP, difficulties planning appointments, the effect of anxiety and sensory issues,[21] trouble following up on care, difficulty identifying and reporting pain, fear, embarrassment or frustration, [22] and not feeling understood.[23] Similar barriers have been identified by autistic clients accessing counsellors, including practitioners misunderstanding or not believing them, a lack of neurodiversity affirming knowledge amongst clinicians, and a lack of broader knowledge in areas related to autism, such as gender, and co-occurring conditions.[24] Autistic people’s experiences within the mental health system has frequently been found to be alienating and counter-productive, often due to a system that fails to observe autistic differences.[25]
An example of these barriers is where written information explaining treatment and after care may not be read or absorbed by those struggling with literacy or attention, and difficulties in independently maintaining organisational routines might affect self-management of medication. When the neurodivergent person appears verbally competent, an assumption may be made by the clinician that their client is choosing not to take responsibility for their health care. This belief that the clients’ actions regarding their healthcare are a defiant choice rather than due to executive functioning difficulties can result in detrimental treatment by the clinician.[26]
Autistic adults also reported increased adverse health outcomes that correlated with the difficulties they faced in engaging with healthcare. Some of these outcomes were untreated physical and mental health conditions, not attending specialist referral or screening programmes, requiring more extensive treatment or surgery due to late presentations, and untreated potentially life-threatening conditions.[27] These barriers likely have real consequences, as evidenced in reduced life expectancy, and higher levels of physical and mental health conditions among autistic people.[28]
While there are a variety of studies that have explored the co-occurrence of various mental and physical health conditions with neurodivergence, there remains very little research into appropriate treatment and management strategies. Recent studies within the mental health space have found that neurodiversity-affirming clinical interventions, tailored to the needs of autistic people are urgently required[29] and that further research is needed to determine strength-based interventions that achieve positive outcomes for autistic children and adolescents.[30] At present there does not seem to be many, if any, evidenced-based treatments that have been specifically designed and tested for neurodivergent people.
Regarding physical health conditions, there are some concepts such as The Explain Pain Handbook: Protectometer[31] that seemed well-aligned to Neurodiversity Affirming Practice. The book explains that the pain experience is individualised and that it can be changed. The theory suggests that the more “DIMs—Danger in Me signs” an individual has, the greater the risk of hitting the pain threshold, and the more “SIMs—Safety in Me signs” they have, the lower the risk of hitting that threshold. Therapy then focuses on removing DIMs, then finding, and enhancing SIMs. The understanding that everybody’s experience is unique and therefore treatment needs to be adapted seems supportive of neurodivergent needs, however there has not yet been any research to verify this.
Neurodiversity scholars have explored the idea that thriving and wellbeing are not necessarily at odds with being autistic.[32] It seems that there is currently a lot of advancement needing to occur within healthcare before the majority of neurodivergent people will be able to flourish throughout their lives. Despite many studies confirming the many co-occurring conditions this information is not yet integrated into the mainstream practice of those working with neurodivergent people. Numerous studies have recommended blanket screening for certain conditions when someone is identified as Neurodivergent, yet the reality is individuals are often not even given information regarding their increased risk, let alone being offered assessment for these conditions.
This lack of education for both clinicians and clients, along with the numerous barriers that Neurodivergent individuals experience when accessing healthcare, means that many people live without appropriate diagnosis. This results in many neurodivergent people going without appropriate treatment, suffering with uncontrolled symptoms, and having decreased quality of life. While many physical conditions will remain undiagnosed, it is more common that mental health conditions will be misdiagnosed. Overlapping symptoms and a general lack of understanding regarding the nuance of Neurodivergence means people may be incorrectly diagnosed with a mental health condition without having their neurodivergence ever identified. Given how important neurodiversity affirming strategies are for understanding self, it is likely that those who remain unidentified and incorrectly treated will never fully ‘recover’ or heal.
The discrepancy between current clinical knowledge, practice and treatment, and then the emerging knowledge about the multitude of co-occurring conditions within the Neurodivergent community leaves many at risk of poor quality of life, as well as considerably shorter life expectancy. Unfortunately, it seems that yet again, much of the burden to bring about change will be left to those who are Neurodivergent. Those who are already vulnerable and drained, in part because of current systems that are not designed to be accessible to them. Those who will find a way, because they know how challenging life will remain for so many within the Neurodivergent Community if these hidden conditions and associated issues remain unresolved.
Glossary
Dysautonomia is a group of conditions where the autonomic nervous system (ANS) is not functioning properly impacting some automatic processes that occur such as the respiratory rate, heart rate, blood pressure, digestion, sexual arousal, and temperature regulation. For more information please see http://www.dysautonomiainternational.org/index.php
Mast Cell Activation Disorder (MCAS) is a malfunctioning of part of the immune system, where a type of immune cell (mast cells) release an excess of inflammatory chemicals such as histamine, causing allergy-like symptoms throughout the body. For more information please see https://www.mastcellaction.org/about-mcas
Connective Tissue is found all over the body and has a wide variety of functions. It is responsible for support, protection, insulating, storage of reserve fuel, and transporting substances. Different types of connective tissue have different roles including holding organs in place and linking bones together at joints.
Ehlers-Danlos Syndromes (EDS) are a group of connective tissue disorders. As there is a wide range of EDS types there is a wide variety of symptoms, each type of EDS has the potential for disability and negative impact on the quality of life in some individuals. For more information please see https://www.ehlersdanlosaus.com/
Fibromyalgia is a common condition in which people experience symptoms that include widespread pain and tenderness in the body, often accompanied by fatigue and problems with memory and concentration. For more information please see https://msk.org.au/fibromyalgia/
Endometriosis is where cells like the ones in the lining of the uterus are found elsewhere in the body. Each month these cells build up and then break down but with no way for this blood to escape the body. This can result in debilitating pain that is often not controllable with pain killers. For more information please see https://endometriosisaustralia.org/
Premenstrual Dysphoric Disorder (PMDD) is a hormonal health condition that causes clinically significant mental health symptoms, and uncomfortable physical symptoms in the week prior to onset of a period. This disabling condition seriously impacts daily life for those affected. For more information please see https://www.jeanhailes.org.au/news/pms-and-pmdd-and-you
Rejection Sensitive Dysphoria (RSD) is when a person experiences severe emotional pain because of a failure or feeling rejected. People with RSD are also more likely to interpret vague interactions as. It is often experienced by people who also have ADHD. For more information please see https://www.additudemag.com/rejection-sensitive-dysphoria-adhd-emotional-dysregulation/
Avoidant/Restrictive Food Intake Disorder (ARFID) is an eating or feeding disorder characterised by a persistent and disturbed pattern of feeding or eating that leads to a failure to meet nutritional/energy needs. For more information please see https://www.eatingdisorders.org.au/eating-disorders-a-z/arfid/
Dyslexia is a term that refers to difficulty in acquiring and processing language. People with dyslexia have difficulty connecting letters they see on a page with the sounds they make. As a result, reading becomes slow and effortful and is not a fluent process for them.
Dysgraphia is a term used to describe difficulties with putting one’s thoughts on to paper. Problems with writing can include difficulties with spelling, grammar, punctuation, and handwriting.
Dyscalculia is a term used to describe difficulties learning number related concepts or using the symbols and functions to perform math calculations. This can result in difficulties with number sense, math calculations, math reasoning and math problem solving.
Invisible Disability is a term that captures a range of disabilities that are not visible from the outside, yet can limit or challenge a person’s movement, sense, or activities. These include chronic health conditions, mental health, or neurodiversity.
Intersectionality refers to the ways in which different aspects of a person’s identity can expose them to overlapping forms of discrimination and marginalisation. When these aspects or characteristics combine people find it harder to get the help they need due to systemic barriers.
Masking or Camouflaging are terms used to explain strategies used by autistic individuals in everyday life to help them cope in social situations and to try and “fit in” with the social norms of the neurotypical majority. For more information please see https://www.autism.org.uk/advice-and-guidance/professional-practice/autistic-masking
Neurodiversity Affirming Practice recognises and accepts the unique differences and strengths of individuals with neurological differences. It rejects the idea that neurodivergent people need “fixing” instead focusing on creating more inclusive and supportive environments for all individuals.
References
[1] Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. 2022. https://doi.org/10.3389/fpsyt.2021.786916
[2] The Links Between Fibromyalgia, Hypermobility and Neurodivergence. 2022. https://doi.org/10.17925/RMD.2022.1.1.3,
[3] Pathways to Anxiety and Depression in Autistic Adolescents and Adults. 2023. http://dx.doi.org/10.1155/2023/5575932
[4] Eating disorders and neurodivergence. 2023. https://withinhealth.com/learn/articles/eating-disorders-and-neurodivergence
[5] Ehlers-Danlos Syndrome in the Field of Psychiatry: A Review. 2022. https://doi.org/10.3389/fpsyt.2021.803898
[6] https://chadd.org/about-adhd/co-occuring-conditions/
[7] Everyday life consequences of substance use in adult patients with a substance use disorder (SUD) and co-occurring attention deficit/hyperactivity disorder (ADHD) or autism spectrum disorder (ASD): a patient’s perspective. 2014. https://doi.org/10.1186/s12888-014-0264-1
[8] Australian evidence-based clinical practice guideline for Attention Deficit Hyperactivity. 2022. https://adhdguideline.aadpa.com.au/wp-content/uploads/2022/10/ADHD-Clinical-Practice-Guide-041022.pdf
[9] PMDD, Autism, and ADHD: The Hushed Comorbidity. 2023. https://www.additudemag.com/pmdd-autism-adhd/
[10] Endometriosis and Women with hEDS. 2023. https://www.actifypt.com/post/endometriosis-and-heds
[11] https://www.educalm.co.uk/post/neurodiversity-and-endometriosis
[12] Managing endometriosis: a cross-sectional survey of women in Australia. 2020. https://doi.org/10.1080/0167482X.2020.1825374
[13]https://www.inneg.co.uk/2023/04/03/autism-trauma-and-neurodivergence-aspects-to-consider-in-personal-injury-claims/
[14] [15] https://neurodivergentinsights.com/misdiagnosis-monday
[16] “Having All of Your Internal Resources Exhausted Beyond Measure and Being Left with No Clean-Up Crew”: Defining Autistic Burnout. 2020. https://doi.org/10.1089/aut.2019.0079
[17] [19] Co-Occurring Physical Health Challenges in Neurodivergent Children and Young People: A Topical Review and Recommendation. 2023. https://www.tandfonline.com/doi/full/10.1080/13575279.2022.2149471
[18] [22] Barriers to healthcare for Australian autistic adults. 2023. https://doi.org/10.1177/13623613231168444
[20] https://www.usersnews.com.au/home/drug-use-disability-healthcare
[21] [28]Barriers to healthcare and self-reported adverse outcomes for autistic adults: A cross-sectional study. 2022. https://doi.org/10.1136/bmjopen-2021-056904
[23] [27]Barriers to healthcare for autistic adults: Consequences & policy implications. A cross-sectional study. 2020. https://doi.org/10.1136/bmjopen-2021-056904
[24] ‘You need support, validation, good coping skills. You need and deserve acceptance”: Autistic Adult Experiences of Counselling. 2020. www.autisticmentalhealth.uk/counsellingreport
[25] [29] [32] Addressing the autism mental health crisis: the potential of phenomenology in neurodiversity-affirming clinical practices. 2023. https://doi.org/10.3389/fpsyg.2023.1225152
[26] Neurodiversity at work: a biopsychosocial model and the impact on working adults. 2020. https://doi.org/10.1093/bmb/ldaa021
[30] Neurodiversity in Practice: a Conceptual Model of Autistic Strengths and Potential Mechanisms of Change to Support Positive Mental Health and Wellbeing in Autistic Children and Adolescents. 2023. https://doi.org/10.1007/s41252-023-00348-z
[31] G. Lorimer Moseley & David S. Butler. 2015. The Explain Pain Handbook: Protectometer